

Omega 3’s are a type of fatty acid found as certain sources of polyunsaturated fat. These are considered essential fats in that humans cannot produce them endogenously through the breakdown of other dietary fats. They must be consumed through diet alone. The three main types of Omega 3’s are known as DHA, EPA and ALA. The first two are long-chain fatty acids that are primarily found in seafood and marine algae while the latter is short-chain and is most commonly from plants sources. The human body generally uses ALA as a source of energy, although conversion to EPA and DHA does occur and the conversion rate may differ from person to person.

Physical Well-being
There are many conflicting studies about Omega 3 intake when it comes to cardiovascular health and a definitive conclusion isn’t wholly agreed upon. There is good evidence to support a protective benefit against cardiovascular diseases but on the contrary, there are also plenty of studies which don’t observe any benefit at all. Let’s start by going over the latter.
A systematic review and meta-analysis was conducted in 2012 regarding omega 3 supplementation which included 3,635 citations and twenty studies of 68,680 patients. This study observed no benefit in regards to all-cause mortality, cardiac death, myocardial infarction and stroke when all studies were considered (Rizos, 2012). Another, more recent study reviewed twenty-one randomized control trials that assessed omega 3 supplementation and its effects on overall mortality and cardiovascular health and found no consistent benefit (Rizos, 2017). Another 2012 meta-analysis which analyzed fourteen randomized, double blind, placebo controlled studies and included a total of 20,485 patients also failed to find any secondary preventative benefits for cardiovascular disease (Kwac, 2012).
There is still some high quality research suggesting that intake of DHA and EPA may provide some cardiovascular benefit. A 2017 review and meta analysis which included eighteen randomized control trials and sixteen prospective cohort studies concluded that higher EPA and DHA intake from food or supplements may result in reduced coronary heart disease risk, with a greater benefit seen in higher-risk subjects (Alexander, 2017)(Marik, 2009). These findings are in complete opposition to some of the above-mentioned conclusions. Another 2017 review and meta analysis of DHA and EPA supplementation which included fourteen randomized control trials demonstrated a modest reduction in cardiac death between the subjects supplementing with DHA and EPA and the control group (Maki, 2017). Several meta-analyses have also found a small yet statistically significant lowering of blood pressure in most subjects supplementing with omega 3’s (Colussi, 2017).
Omega 3 supplementation in the form of krill oil has shown promising effects in some research regarding lowering inflammatory markers as well (Kidd, 2007). Chronic inflammation is linked to some conditions such as arthritis, diabetes, depression, Alzheimer’s, cancer and heart disease, which may explain the mechanisms in which a cardioprotective effect may occur. More research is needed on this, however.

Mental Well-being
Both DHA and EPA intake has been shown to increase brain function and cognition marginally and exhibits a neuroprotective effect. The combination of the two have demonstrated beneficial effects in subjects with attention deficit/hyperactivity disorder, autism, dyspraxia, dyslexia, aggression, onset of alzheimer’s and dementia, major depressive disorder (MDD) and bipolar disorder with promising evidence in regards to schizophrenia and borderline personality disorder as well. Subjects exhibiting accelerated cognitive decline and impairment also correlate with lower DHA and EPA in their brain tissue. Supplementation to increase these levels has been successfully shown to improve both conditions (Kidd, 2007). A 2015 systematic review and meta-analysis concluded that omega 3 supplementation resulted in an increase in cognition for subjects who were deficient. The same cognitive benefit wasn’t seen in subjects who were not identified as deficient or demonstrated neurodevelopmental disorders (Cooper, 2017). This makes sense because increasing levels of DHA and EPA beyond a healthy level has been shown in multiple other studies to not result in any increased benefits.
Starting at about the age of twenty, brain volume has been observed to continuously shrinks in size. By the age of about eighty, the average person will have a brain size reduced to the size of an average two year old. Increased intake of DHA and EPA in subjects over the course of an eight year study resulted in higher brain volume versus subjects with a lower intake (Alessio, 2014). This is good evidence that increased long chain fatty acid is particularly beneficial for aging individuals.
Concerns of Omega 3 Intake
Most DHA and EPA omega 3 supplements are derived from fish or other aquatic life. Due to the growth of environmental pollutants in the water supply, aquatic life is now contaminated with higher levels than ever of methylmercury and PCB’s. These contaminants bio-accumulate in fat cells and therefore magnify up the food chain (Crinnion, 2011). Predatory aquatic life will contain much higher contaminant bioaccumulation than aquatic plants, for example. Methylmercury and PCB’s have been shown to be detrimental to cognitive and behavioral function, especially in developing children, as well as problems with the immune system, hypothyroidism, and possibly type 2 diabetes (Crinnion, 2011). Some studies even show PCB’s to cause an increased risk of stroke, which is indicative of cardiovascular detriments as well (Bergkvist, 2013).
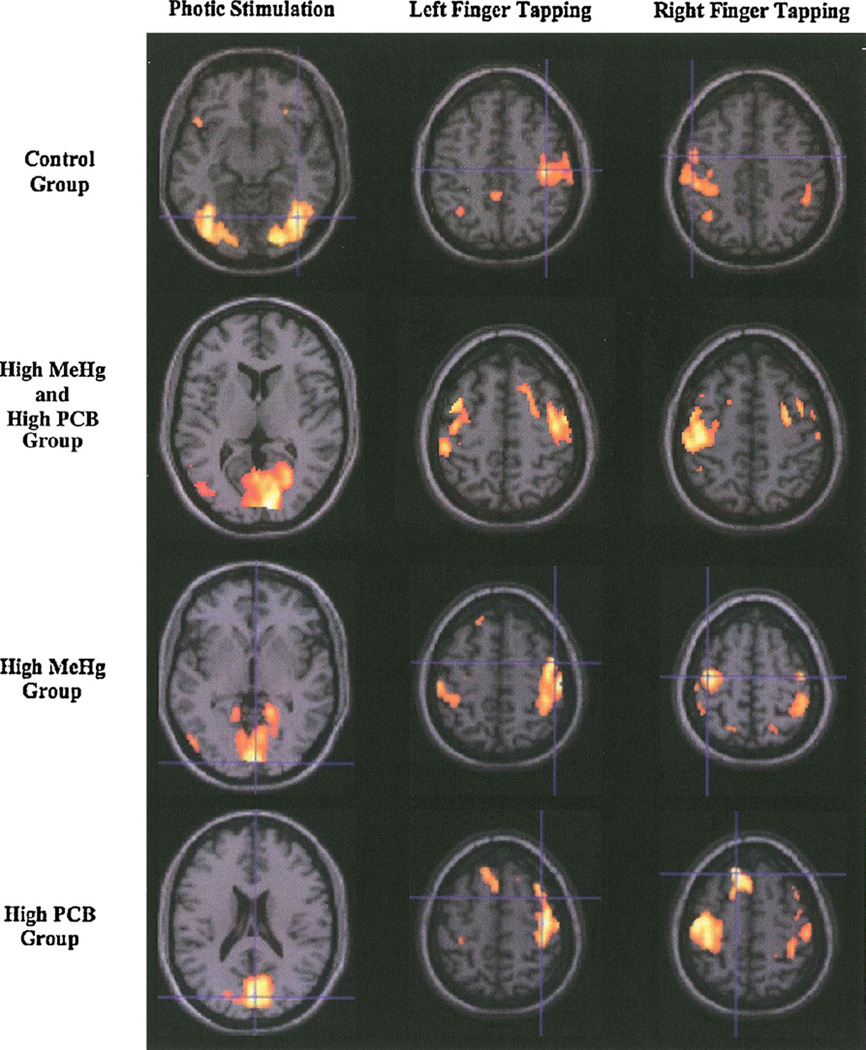
Two groups of fifteen year old boys were divided to compare brain function based on prenatal exposure to methylmercury and PCB’s. One group was low exposure and the other was high exposure. Both groups were given simple visual and physical exercises. The low exposure group demonstrated activation of areas of the brain identified as normal to average, healthy brain activity. However, the high exposure group showed much more varied brain activity and in unusual areas (White, 2011).
High levels of prenatal mercury exposure has been shown to result in slightly lower IQ scores later on in life, and the greater the amount of mercury exposure, the lower the IQ score result (Axelrad, 2007). One study identified up to a ten point decrease in IQ score in subjects whose mothers consumed fish species highest in pollutants during pregnancy (Zeilmaker, 2013).

When accounting for the increased level of contaminants in aquatic life and supplements derived from them, the overall effect may actually be negated. One study compared a healthy population consuming increased omega 3’s with low exposure to environmental contaminants to a group consuming high amounts of fish in an area with high levels of contaminants. The increased omega 3 intake showed a slight benefit to serum triglyceride levels and inflammation in the control group but the high exposure group didn’t see the hypothesized benefit with insulin resistance and arterial stiffness. This was expected to be because of the high level of contaminants, specifically (Torunen, 2013). The growing amount of pollutants in the water supply will likely only exacerbate these issues in the future (Oken, 2012). 
Fish and seafood consumption, including many omega 3 supplements, has an obvious impact on aquatic life populations which in turn leads to concerns over sustainability (Greene, 2013). Switching to supplements derived from marine algae is much more beneficial to the aquatic ecosystem, sustainable, and healthier due to lower levels of environmental contaminants.
ALA Conversion
The human body is believed to have a limited capacity for conversion of dietary ALA sourced omega 3’s to DHA and EPA. The conversion factor seems to differ greatly from person to person. In general, women seem to exhibit a greater ability to convert ALA in the body than men (Burdge, 2017). However, a 2010 paper examining differences in different dietary patterns and circulating DHA and EPA found only a nominal difference between fish eaters and vegetarians/vegans. Substantial differences in long chain fatty acid consumption was observed between groups, but levels in the body were not much different. This suggests higher levels of ALA conversion to DHA and EPA in the body when intake of the latter are lower (Welch, 2010). Another study conducted by Rosell in 2005 also observed the same occurrence. There are no established recommendations for consumption of omega 3’s in a plant based diet, but one study suggests vegetarians/vegans double intake of ALA for optimal conversion (Saunders, 2013). ALA consumption will likely already be much higher in a plant based diet, so it may just be helpful to make sure to get some from a quality source such as flaxseeds, hemp seeds, and/or chia seeds everyday.
Normal aging seems to decrease the amount of ALA converted to EPA and DHA in the body. Individuals following a plant based diet may have more of a reason to supplement with a plant-based long-chain fatty acid supplement for optimal brain health and maybe consume more ALA as well (Saunders, 2013).
Omega 3 Intake in a Plant-based Diet
According to one study, people who don’t eat fish may be under the recommended healthy amount of long chain omega 3 fatty acids. It seems that there is a threshold for optimal intake that, when exceeded, results in no further benefits, but when below that threshold, seems to result in accelerated brain loss. Nearly two thirds of vegans may fall below the optimal amount, although those following a standard american diet didn’t seem to do much better either. A 254 miligram supplementation of long chain omega 3’s over a four month period raises deficient subjects over the threshold marker. A plant-based diet revolving mostly around whole foods inherently has a major advantage over many other diets when it comes to Omega 6 versus Omega 3 intake. Most people following a standard western diets will have vastly higher omega 6 intake than is recommended. The optimal ratio is currently identified to be a 1:1 to 4:1 for omega 6 to omega 3 respectively. In other words, omega 6 and omega 3 intake should be roughly equivalent or omega 6 intake should be four to five times higher than omega 3, at the most. Individuals following a standard western diet have an average ratio around 10:1 to as high as 20:1 (Simopoulos, 2016). A ratio this imbalanced has been shown to result in higher risk of mental health disorders and several diseases such as heart disease and obesity.It’s commonly known that fish are generally high in DHA and EPA omega 3’s but where are they getting theirs from? The origin in aquatic ecosystems actually starts from algae. Aquatic algae naturally contains high levels of these omega 3 fatty acids without the bioaccumulation of harmful pollutants such as PCB’s and methylmercury that are so prevalent in fish, especially predatory fish. In clinical trials, microalgae oil demonstrates comparable effects with fish-sourced omega 3 supplements (Doughman, 2007). Aquatic plants also have a much lower level of pollutants compared to fish and other aquatic life so it’s a win-win. Based on the research, I think it’s safe to say that supplements derived from marine algae is the best source of DHA and EPA for everyone; not just vegans. A 250 milligram total dose of algae-derived DHA and EPA seems to sufficient in raising serum levels optimally in most people (Saunders, 2013)(Sarter, 2015).
Summary
If you made it through this whole article, it’s obvious that there’s a lot of conflicting evidence on the subject of omega 3’s. The benefits for cardiovascular health aren’t completely substantiated. There’s some evidence that there may be a small cardioprotective effect as well as well as a possible benefit with inflammatory markers and blood pressure. There seems to be more evidence in favor of a neuroprotective effect and reducing the risk and severity of various neurological disorders. Higher DHA and EPA also seem to delay the loss of brain volume and increase cognition in aging individuals. However, the high exposure of environmental pollutants such as methylmercury and PCB’s in aquatic life, which is usually where most DHA and EPA supplements are derived from, may very well confound some of these possible benefits. These contaminants undoubtedly cause harm in the human body and will offset any possible benefit from the long chain fatty acids. Marine algae derived DHA and EPA contain the least amount of contaminants since it’s at the base of the food chain and bioaccumulation is an issue in fish and other aquatic life. Relying on conversion of ALA short-chain fatty acid to its long-chain counterparts may not be reliable for everyone following a plant-based diet. Although there’s some evidence showing that ALA conversion increases sufficiently when intake of DHA and EPA decreases, there’s variables such as age and sex that may not make it a safe bet to rely on for everyone. For these reasons, I think it’s safe to recommend algae supplements specifically to everyone seeking the possible benefits of DHA and EPA. A 250 milligram total daily dose of both DHA and EPA has been shown to optimize serum levels in vegans, so this is a safe, general recommendation to anyone.